
How to Tell the Difference Between Nummular Eczema and Ringworm
It’s often difficult to distinguish between nummular eczema and ringworm, so it’s always best to be evaluated by a dermatologist, say experts.
Published On: Aug 4, 2015
Last Updated On: Jul 15, 2021
Dear Dr. Lerner,
I’ve had an unbearable itch all over my body, seen premier dermatologists dozens of times, yet the itch never gets better. I apply creams and take a bunch of medications, which doctors say may be contributing to the itchiness I feel. I can’t tell you how horrible it is. I think that these creams help treat the symptoms, but not the disease or allergy itself. I think it’s killing me when it is really bad. Please, please help me. Please, I can’t stand it anymore.
The above letter is typical of the requests I get from my eczema patients. They share this common thread: treat my itch. While histamine on the skin triggers the sensation of a pure itch, the itch caused by atopic dermatitis often moves beyond itch, to include a pricking, burning and sometimes-painful component. Yet, despite being a universally experienced symptom, no one knows why we have the itch or what we gain from it.
There are a few possible considerations. Most eczema drugs target the immune system, but the itch is some-thing that could be addressed by targeting the nervous system—because if nerves were blocked, then patients wouldn’t feel the itch. And that raises the question, if you block the nerves, will the rash go away?
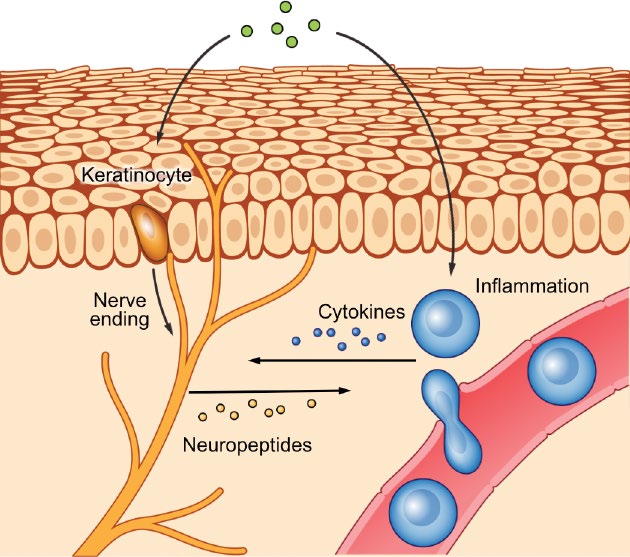
There’s a little bit of inflammation that’s always present even in the skin that’s not involved with the itch. So maybe the nerves are kind of turned on, and maybe the immune system is also turned on. And the reality is all of these things are talking to each other in a complicated network of systems.
Being born as the offspring of two dermatologists didn’t spare me from having atopic dermatitis. I know firsthand about the itch.
As an adult in the academic world, my job demanded I be on the phone all the time, and I developed what I called “phonodermatitis” — recurring eczema on the left side of my ear and face. Now, the logical thing would be to tell a patient to hold the phone on the other ear while talking, but humans are creatures of habit and I was used to holding the phone a certain way. These are real issues. I feel your itch.
In my work, I wanted to do more than hold patients’ hands as they go through their journey with eczema; I wanted to contribute to the development of new things, such as ways of alleviating the itch.
The itch is going to be cured! This is not some hope for the future; the developments are happening right now.
Many people have tried creams or steroids to relieve the itch, but lesser-known treatments that affect the nervous system, called neuromodulators, can also be used. These treatments shouldn’t necessarily be used in children, but they can be used by adults.
One type of neuromodulators are the selective serotonin reuptake inhibitors (SSRIs), which people tend to think of as antidepressants — and they can be — but they can also be very helpful in addressing certain cases of itch.
Other neuromodulators include serotonin-norepinephrine reuptake inhibitors (SNRIs), gabapentin, pregabalin, and the medicines aprepitant, amantadine, and memantine.
While these and related compounds aren’t suitable for many cases of atopic dermatitis, they can be useful for some. If you want to pursue these options, but are working with a doctor who is not knowledgeable about neuromodulator treatments, follow up with another doctor who may be able to consider whether you are a candidate for this type of treatment.
The complete list of drugs approved to treat itch is a short one, comprising topical steroids, antihistamines, and oclacitinib. But antihistamines don’t often work because histamines are not involved in most itches, and oclacitinib is actually a treatment for dogs, so the short list becomes even more blighted.
The good news is that although there is a dearth of drugs to treat itch today, the medical community — including drug companies, the NIH, and the academic community — is working to provide new treatment options.
Some promising treatments are not yet approved to treat itch. The neuromodulators previously mentioned are among them. We are discovering that cannabis may be another.
Dr. Sarina Elmariah, a neuroscientist and dermatologist with whom I work, had a patient report that smoking marijuana helped relieve the itch brought on by his atopic dermatitis. Another patient who had an extremely difficult problem with treatment and who wasn’t responsive to anything, including the neuromodulators that I mentioned, saw beneficial change after using medical cannabis in a state in which it’s legal.
One Massachusetts General Hospital patient with a horrible itch would get the problem treated in the hospital, then go home only to have it exacerbate again. Wash, rinse, repeat. But after a family member passed away, the pattern ceased, which may indicate that the way in which we handle interpersonal relationships contribute to the itch factor.
Although we don’t know much about how to treat itch, we do know a bit about how itch works.
Eczema itch happens when things outside the body, such as allergens or irritants, trigger the immune and nervous systems.
Mast cells in the skin release histamine — a small molecule that interacts with a histamine receptor that’s present on the nerve in the skin. This interaction sends a signal to the spinal cord and to the brain. Your brain then says, “You’re itchy, go ahead and scratch.” And of course, the logical response is to simply resist that message by not scratching, but since it’s near impossible not to scratch, we try to tell patients to try to scratch less or squeeze a piece of rubber as a way of getting that release.
In order to learn more about how itch works outside of histamine, we turned to an age-old substance — itching powder. Because it really causes itch, yet doesn’t work through histamine, we reopened a long-closed inquiry about the factor in itching powder that creates an itchy and burning sensation on skin.
Itching powder is actually derived from a tropical bean plant that grows all around the world. The plant yields pods covered with little hairs. We removed the hairs from the pods in the lab and extracted what we hoped would be the active ingredient for itching powder.
Because I like to be my own guinea pig, I tested them on myself by putting the hairs in solvents of different kinds, including water and alcohol.
We worked to isolate the active component, a protein, identify its amino acids, and clone its gene so we could reproduce it. After finding the active component, we could see that it was similar to a gene that is also in people, where it also causes itch.
A couple of companies are working on treatments related to this. One idea involves blocking that activity, which could serve as way to treat itch.
By using cortisones, or steroids, we can block immune cells and inflammation, but cortisones have downsides, as we all know.
Another drug is tacrolimus. It can block inflammation without the side-effects of steroids, and can be useful for treating itch.
The main skin cell is a keratinocyte that sends and receives signals to and from nerve fibers in the skin. And there’s a particular nerve fiber called a C-fiber that goes to an area outside the spinal cord, then into the spinal cord where it links up with other nerves that travel up the spinal cord to the brain where the itch-scratch cycle is produced.
So we are beginning to explore whether we can block the right cytokine without creating problems that would occur when other things are shut down. The question is, are there certain cytokines that may be better to block than others?
Dupilumab is certainly a good place to start. It hits interleukin 4. Genentech has a drug that blocks an antibody called IgE, which is involved in allergy and hives.
Interleukin 17 is really important in psoriasis, interleukin 31 is important in itch. Perhaps blocking interleukin 31 will help to treat itch.
Another cytokine is TSLP, thymic stromal lymphopoietin, which is made by T cells, but interacts with receptors on the nerves. Other receptors for cytokines that you’ll hear more about in the future include TRPs, or transient receptor potential channels. Huge progress has been reported very recently in high-profile journals in regard to TRP A1 and TRPV3. These TRPs are present on the keratinocytes and on the nerve fibers. Staphylococcus is known to interact with one of these TRP channels to directly cause pain and possibly cause some degree of itching.
Voltage-gated sodium channels are on nerves, and when activated, this so-called “action potential” is involved with transmitting nerve signals.
If we could block the nerve fiber and the action potential, the feeling of itch would be blocked. I think that a lot of rashes would go away if the patient didn’t feel the itch. Blocking the nerves might allow us to escape from the itch-scratch cycle.
Brain natriuretic peptide or BNP and gastrin-releasing peptide or GRP are two more things that turn on itch, so it may be possible that blocking these would be helpful.
Another thing to consider is the natural balance in the way our bodies work. When we manipulate one thing, a counter balance occurs.
It turns out that our bodies are actually stocked with endogenous molecules, such as dynorphin, that tone down the itch. This begs the question, rather than blocking nerves or cytokines, can we take advantage of things that are already inside us in order to tone down itch?
Though itch is complicated, mechanisms of itch are being clarified and researchers are looking to find out whether drugs that block nerves would work to cease itch. New drugs are coming.
Very recently, we have begun to inject mice with a version of the anesthetic lidocaine, while at the same time giving them atopic dermatitis.
We are discovering with these studies in the lab that we can pretreat some patients’ itchy eczema with topical lidocaine, and prevent the development of the itch. We are learning that in the presence of lidocaine not only do mice scratch less, they don’t get a rash. So for some patients who can feel a flare-up coming on, we may be able to intervene.
All in all, I think the future is bright in regard to clarifying the mechanisms of itch and developing new ways to block these mechanisms, so patients, like the gentleman whose letter I shared at the beginning of this article, can find the relief they so desperately seek.
Etha n Lerner, M.D., Ph.D., is an associate professor of dermatology at Harvard Medical School and studies the mechanisms itch at Massachusetts General Hospital.
n Lerner, M.D., Ph.D., is an associate professor of dermatology at Harvard Medical School and studies the mechanisms itch at Massachusetts General Hospital.
It’s often difficult to distinguish between nummular eczema and ringworm, so it’s always best to be evaluated by a dermatologist, say experts.

Karin Stoddart, 20, a college student from Seattle, finally has her eczema under control after battling with two insurance companies to stay on her doctor-prescribed medication.

Learn which plants won’t irritate your eczema — and can also help purify the air in your home.

Christina Crowley, from Berkeley, California, shares how she became a NEA board member — recently NEA’s Board Chair in 2023 — as well as a donor and Itching for a Cure fundraiser.


Evidence-based articles, expert-sourced lifestyle tips and stories from your community.